
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Neverending Covid-19 Coronavirus
- Thread starter RenegadeMonster
- Start date
LeSamourai
Well-Known Member
Great, now I gotta stop eating cuy?! This fascism will not stand
When we get to the food chapter in our textbook, I love the look on my students' faces when I show them that guinea pigs only exist because people in South America bred them as food.
I've never had it, but I did each carpincho (capybara) when it was served to me a few times in northern Argentina.
Last edited:
dhodo
Well-Known Member
I tried it once and enjoyed it, but came down with a pretty crummy gastrointestinal infection the next day, so kinda hard to fully associate it with a positive experience. Who knows what it really came from though. Probably something else.When we get to the food chapter in our textbook, I love the look on my students' faces when I show them that guinea pigs only exist because people in South American bred them as food.
I've never had it, but I did each carpincho (capybara) when it was served to me a few times in northern Argentina.
mrjoshuamccormack
Active Member
This is just sad to me. From what I've read, there are a lot of requirements in order to get an organ transplant, including vaccinations, but this guy just refuses to get a COVID shot:
Upstate man taken off wait list for kidney transplant for not getting vaccinated for COVID-19
Upstate man taken off wait list for kidney transplant for not getting vaccinated for COVID-19
Hhabelt
Active Member
What is? Paywalls being removed from potentially life altering content?
*click*
Nope. That's not it.
I'm sorry. That appears to be great news.
Well, we think that Omicron mutated in rat populations and then reinfected humans, so this shouldn't be too surprising. This virus, y'all...
Transmission of SARS-CoV-2 (Variant Delta) from Pet Hamsters to Humans and Onward Human Propagation of the Adapted Strain: A Case Study

Transmission of SARS-CoV-2 (Variant Delta) from Pet Hamsters to Humans and Onward Human Propagation of the Adapted Strain: A Case Study
Background: Transmission of SARS-CoV-2 from humans to other mammals, including pet animals, has been reported. However, with the exception of farmed mink, therepapers.ssrn.com

I've eaten nutria before and that's the closest I've gotten to eating rodents.When we get to the food chapter in our textbook, I love the look on my students' faces when I show them that guinea pigs only exist because people in South America bred them as food.
I've never had it, but I did each carpincho (capybara) when it was served to me a few times in northern Argentina.
Sorry, it was readable in full via Apple News last night but seems to be paywalled thru WaPo for no reason.
The upshot is that 2 doses is safe for kids under 5. There’s a lack of immune response in ages 2-5 that will probably require a 3rd shot, but before you can get a third shot, you need the first two, so…why not start getting that rolled out?
Huge news for families if this plays out. The most recent updates I had seen before this were that we might be well into summer before it might be available.
I thought the WaPo made all stories about Covid-19 public / not behind the paywall. Did they change this recently? Or does the paywall trigger after X amount of articles a month available for free.
No paywall for me when following the link on my Mac. And it's opening Chrome, not Apple News.
I get paywalled. I'm on a PC and I'm using Chrome. It could be due to the number of free articles I no longer have.I thought the WaPo made all stories about Covid-19 public / not behind the paywall. Did they change this recently? Or does the paywall trigger after X amount of articles a month available for free.
No paywall for me when following the link on my Mac. And it's opening Chrome, not Apple News.
WHAT IS THIS HOT GARBAGE???
/cloudfront-us-east-1.images.arcpublishing.com/gray/AJOPU7HETJBAHMK7N5GTQ2QFVA.jpg)
 www.kttc.com
www.kttc.com
So, I had to go to the study and read the methods y'all, because bad science is my kryptonite.
After screening based on the title, 1,048 papers remained. These papers were manually screened by answering two questions: 1. Does the study measure the effect of lockdowns on mortality? 2. Does the study use an empirical ex post difference-in-difference approach (see eligibility criteria below)? Studies to which we could not answer “yes” to both questions were excluded. When in doubt, we made the assessment based on reading the full paper, and in some cases, we consulted with colleagues.11
We distinguish between two methods used to establish a relationship (or lack thereof) between mortality rates and lockdown policies. The first uses registered cross-sectional mortality data. These are ex post studies. The second method uses simulated data on mortality and infection rates. 15 These are ex ante studies. We include all studies using a counterfactual difference-in-difference approach from the former group but disregard all ex ante studies, as the results from these studies are determined by model assumptions and calibrations. Our limitation to studies using a “counterfactual difference-in-difference approach” means that we exclude all studies where the counterfactual is based on forecasting (such as a SIR-model) rather than derived from a difference-in-difference approach. This excludes studies like Duchemin et al. (2020) and Matzinger and Skinner (2020). We also exclude all studies based on interrupted time series designs that simply compare the situation before and after lockdown, as the effect of lockdowns in these studies might contain time-dependent shifts, such as seasonality. This excludes studies like Bakolis et al. (2021) and Siedner et al. (2020).
Given our criteria, we exclude the much-cited paper by Flaxman et al. (2020), which claimed that lockdowns saved three million lives in Europe. Flaxman et al. assume that the pandemic would follow an epidemiological curve unless countries locked down. However, this assumption means that the only interpretation possible for the empirical results is that lockdowns are the only thing that matters, even if other factors like season, behavior etc. caused the observed change in the reproduction rate, Rt. Flaxman et al. are aware of this and state that “our parametric form of Rt assumes that changes in Rt are an immediate response to interventions rather than gradual changes in behavior.” Flaxman et al. illustrate how problematic it is to force data to fit a certain model if you want to infer the effect of lockdowns on COVID-19 mortality.
https://sites.krieger.jhu.edu/iae/f...ffects-of-Lockdowns-on-COVID-19-Mortality.pdf
^^ So basically, they had a ton of papers. They weeded out a ton of papers. And they also chose not to use papers that assumed the virus would have spread parabolically among a population because somehow SOMEHOW short term lockdowns which were only supposed to happen for a couple of months, can somehow be influenced by seasonality and gradual human behavior changes due to living in a pandemic. Sure, let's weed out all the papers that "simply compare the situation before and after lockdown" because those are BS due to "time dependent shifts like seasonality". So we can't look at these papers because people behave differently in winter than they do in spring/summer is what they are saying. We cannot just take observational measurements and interpolate from there. We can't take Asian countries that opted for lockdowns and look at mortality rates compared to the West, because SUMMER IS DIFFERENT THAN WINTER. Instead, we are going to take a ton of BS postulation, thus the inclusion of "simulated data on mortality and infection rates. So instead of using REAL data on actual mortality rates of countries that locked down vs no because of seasons, they are going to use studies with simulated data. I don't know if I can read anymore and I'm only on page 9.
I swear this was funded by corporate America to justify keeping people in unsafe working conditions. That's the only thing I see this study being good for.
Johns Hopkins study reveals COVID-19 lockdowns had little impact
A Johns Hopkins University study finds COVID-19 lockdowns did little to save lives in the United States and Europe.
So, I had to go to the study and read the methods y'all, because bad science is my kryptonite.
After screening based on the title, 1,048 papers remained. These papers were manually screened by answering two questions: 1. Does the study measure the effect of lockdowns on mortality? 2. Does the study use an empirical ex post difference-in-difference approach (see eligibility criteria below)? Studies to which we could not answer “yes” to both questions were excluded. When in doubt, we made the assessment based on reading the full paper, and in some cases, we consulted with colleagues.11
We distinguish between two methods used to establish a relationship (or lack thereof) between mortality rates and lockdown policies. The first uses registered cross-sectional mortality data. These are ex post studies. The second method uses simulated data on mortality and infection rates. 15 These are ex ante studies. We include all studies using a counterfactual difference-in-difference approach from the former group but disregard all ex ante studies, as the results from these studies are determined by model assumptions and calibrations. Our limitation to studies using a “counterfactual difference-in-difference approach” means that we exclude all studies where the counterfactual is based on forecasting (such as a SIR-model) rather than derived from a difference-in-difference approach. This excludes studies like Duchemin et al. (2020) and Matzinger and Skinner (2020). We also exclude all studies based on interrupted time series designs that simply compare the situation before and after lockdown, as the effect of lockdowns in these studies might contain time-dependent shifts, such as seasonality. This excludes studies like Bakolis et al. (2021) and Siedner et al. (2020).
Given our criteria, we exclude the much-cited paper by Flaxman et al. (2020), which claimed that lockdowns saved three million lives in Europe. Flaxman et al. assume that the pandemic would follow an epidemiological curve unless countries locked down. However, this assumption means that the only interpretation possible for the empirical results is that lockdowns are the only thing that matters, even if other factors like season, behavior etc. caused the observed change in the reproduction rate, Rt. Flaxman et al. are aware of this and state that “our parametric form of Rt assumes that changes in Rt are an immediate response to interventions rather than gradual changes in behavior.” Flaxman et al. illustrate how problematic it is to force data to fit a certain model if you want to infer the effect of lockdowns on COVID-19 mortality.
https://sites.krieger.jhu.edu/iae/f...ffects-of-Lockdowns-on-COVID-19-Mortality.pdf
^^ So basically, they had a ton of papers. They weeded out a ton of papers. And they also chose not to use papers that assumed the virus would have spread parabolically among a population because somehow SOMEHOW short term lockdowns which were only supposed to happen for a couple of months, can somehow be influenced by seasonality and gradual human behavior changes due to living in a pandemic. Sure, let's weed out all the papers that "simply compare the situation before and after lockdown" because those are BS due to "time dependent shifts like seasonality". So we can't look at these papers because people behave differently in winter than they do in spring/summer is what they are saying. We cannot just take observational measurements and interpolate from there. We can't take Asian countries that opted for lockdowns and look at mortality rates compared to the West, because SUMMER IS DIFFERENT THAN WINTER. Instead, we are going to take a ton of BS postulation, thus the inclusion of "simulated data on mortality and infection rates. So instead of using REAL data on actual mortality rates of countries that locked down vs no because of seasons, they are going to use studies with simulated data. I don't know if I can read anymore and I'm only on page 9.
I swear this was funded by corporate America to justify keeping people in unsafe working conditions. That's the only thing I see this study being good for.
I'm the same way.So, are throat swabs the new way of testing? That brings back baaaaad memories of my childhood and strep throat tests. Not real good with those...gag reflex is strong in me, I can barely get through a dentist appointment without almost puking.
Can't say I'm surprised. Everything our government does ends up benefiting the wealthy more than the rest of us.
And now the twittersphere has gotten a hold of this horrible study. This is great:WHAT IS THIS HOT GARBAGE???
Johns Hopkins study reveals COVID-19 lockdowns had little impact
A Johns Hopkins University study finds COVID-19 lockdowns did little to save lives in the United States and Europe.
So, I had to go to the study and read the methods y'all, because bad science is my kryptonite.
After screening based on the title, 1,048 papers remained. These papers were manually screened by answering two questions: 1. Does the study measure the effect of lockdowns on mortality? 2. Does the study use an empirical ex post difference-in-difference approach (see eligibility criteria below)? Studies to which we could not answer “yes” to both questions were excluded. When in doubt, we made the assessment based on reading the full paper, and in some cases, we consulted with colleagues.11
We distinguish between two methods used to establish a relationship (or lack thereof) between mortality rates and lockdown policies. The first uses registered cross-sectional mortality data. These are ex post studies. The second method uses simulated data on mortality and infection rates. 15 These are ex ante studies. We include all studies using a counterfactual difference-in-difference approach from the former group but disregard all ex ante studies, as the results from these studies are determined by model assumptions and calibrations. Our limitation to studies using a “counterfactual difference-in-difference approach” means that we exclude all studies where the counterfactual is based on forecasting (such as a SIR-model) rather than derived from a difference-in-difference approach. This excludes studies like Duchemin et al. (2020) and Matzinger and Skinner (2020). We also exclude all studies based on interrupted time series designs that simply compare the situation before and after lockdown, as the effect of lockdowns in these studies might contain time-dependent shifts, such as seasonality. This excludes studies like Bakolis et al. (2021) and Siedner et al. (2020).
Given our criteria, we exclude the much-cited paper by Flaxman et al. (2020), which claimed that lockdowns saved three million lives in Europe. Flaxman et al. assume that the pandemic would follow an epidemiological curve unless countries locked down. However, this assumption means that the only interpretation possible for the empirical results is that lockdowns are the only thing that matters, even if other factors like season, behavior etc. caused the observed change in the reproduction rate, Rt. Flaxman et al. are aware of this and state that “our parametric form of Rt assumes that changes in Rt are an immediate response to interventions rather than gradual changes in behavior.” Flaxman et al. illustrate how problematic it is to force data to fit a certain model if you want to infer the effect of lockdowns on COVID-19 mortality.
https://sites.krieger.jhu.edu/iae/f...ffects-of-Lockdowns-on-COVID-19-Mortality.pdf
^^ So basically, they had a ton of papers. They weeded out a ton of papers. And they also chose not to use papers that assumed the virus would have spread parabolically among a population because somehow SOMEHOW short term lockdowns which were only supposed to happen for a couple of months, can somehow be influenced by seasonality and gradual human behavior changes due to living in a pandemic. Sure, let's weed out all the papers that "simply compare the situation before and after lockdown" because those are BS due to "time dependent shifts like seasonality". So we can't look at these papers because people behave differently in winter than they do in spring/summer is what they are saying. We cannot just take observational measurements and interpolate from there. We can't take Asian countries that opted for lockdowns and look at mortality rates compared to the West, because SUMMER IS DIFFERENT THAN WINTER. Instead, we are going to take a ton of BS postulation, thus the inclusion of "simulated data on mortality and infection rates. So instead of using REAL data on actual mortality rates of countries that locked down vs no because of seasons, they are going to use studies with simulated data. I don't know if I can read anymore and I'm only on page 9.
I swear this was funded by corporate America to justify keeping people in unsafe working conditions. That's the only thing I see this study being good for.

A ‘stealth’ Omicron subvariant is now spreading, worrying experts
Here's what the science shows so far about whether the BA.2 virus is more transmissible and how it holds up against available vaccines.
What is this all about and can people who already had omicron be reinfected with this variant?
I think I have had Covid twice. The original variant pre vaccine and Omicron. I had read around early 2021 that you can't be reinfected when I was constructing code for breakthrough infections. I thought it was screwy when I read it, and now, they have reluctantly said that yes, you can get reinfected with different variants--much like the flu. If the sub-variant is far enough from the original variant, there is a possibility of reinfection.A ‘stealth’ Omicron subvariant is now spreading, worrying experts
Here's what the science shows so far about whether the BA.2 virus is more transmissible and how it holds up against available vaccines.www.nationalgeographic.com
What is this all about and can people who already had omicron be reinfected with this variant?
Turbo
Well-Known Member
A ‘stealth’ Omicron subvariant is now spreading, worrying experts
Here's what the science shows so far about whether the BA.2 virus is more transmissible and how it holds up against available vaccines.
What is this all about and can people who already had omicron be reinfected with this variant?
Chances are you wouldn't be reinfected if you already had Omicron, because the subvariant is quite similar, but everyone's immune system is different.
Turbo
Well-Known Member
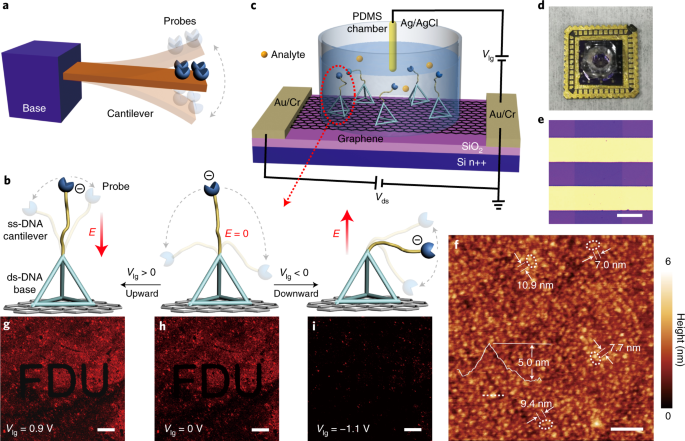
A year and a half ago, I was denigrated for saying that the ideal diagnostic test would be a PCR-less COVID test, so results could be obtained quickly.
Since it's a new technology, it's still early to know how useful it will be in the field, but here it is.
 www.nature.com
www.nature.com
Since it's a new technology, it's still early to know how useful it will be in the field, but here it is.
Rapid and ultrasensitive electromechanical detection of ions, biomolecules and SARS-CoV-2 RNA in unamplified samples - Nature Biomedical Engineering
A self-assembled DNA-based system immobilized on a liquid-gated graphene field-effect transistor can electromechanically detect ultralow levels of unamplified ions, nucleic acids, small molecules and proteins in biofluids.
www.nature.com
Max Sterling
Well-Known Member
The Canadian Olympic Womens Hockey team won their match against the US while wearing N95 masks the entire time.
Don't know why a bunch of manly truck drivers and skeets are having such a hard time with it.
Don't know why a bunch of manly truck drivers and skeets are having such a hard time with it.